EXBLIFEP® / ORBLICEF™
Cefepime 2g + Enmetazobactam 0.5g
IV Infusion

The first Invented in India and Globally Approved Antibiotic, by Orchid Pharma
This is the story of how Orchid Pharma's scientists in 2006 invented a New-Chemical-Entity that became India's first globally approved Anti-infective New Entity (NCE) and how that molecule is now changing the standard of care for drug-resistant infections worldwide.
Developed to serve as a critical carbapenem-sparing option for ESBL producing Gram Negative Bacterial infections Gram-negative infections, it is designed for settings where ESBL-producing Enterobacteriaceae are endemic.
Scroll through the timeline to follow the journey and understand the science at every step.
The Growing Silent Pandemic of Antimicrobial Resistance (AMR)
Before the Solution, Understand the Crisis
In the early 2000s, something alarming began happening inside hospital wards across the world, and India was at the epicenter. Gram-negative bacteria such as Escherichia coli and Klebsiella pneumoniae, normally harmless commensals, began acquiring resistance to nearly every available antibiotic. Today, data from the National Antimicrobial Surveillance Network (NARS-Net) confirms that resistance to third-generation cephalosporins is now the norm, not the exception, in India.
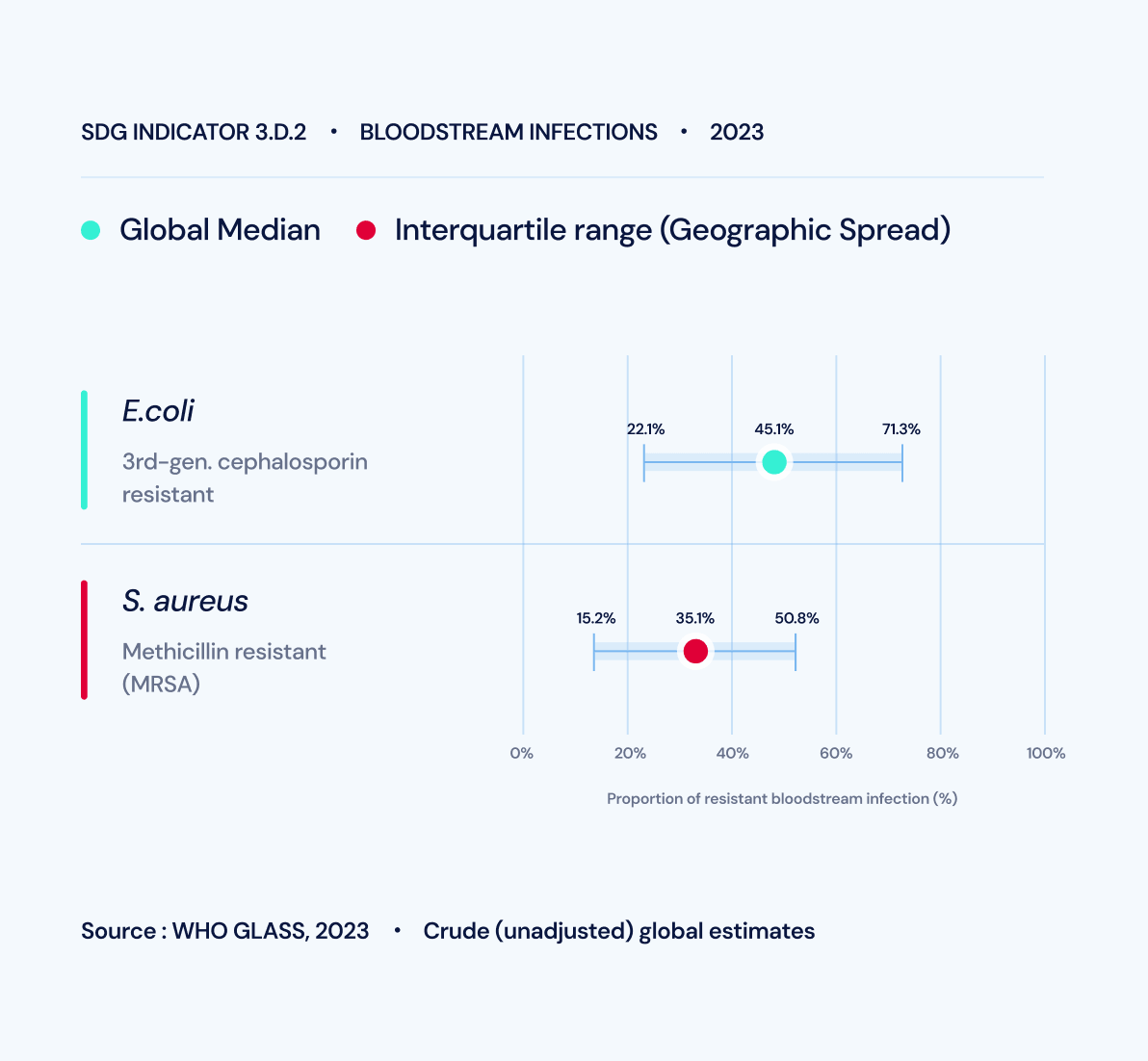
The mechanism driving this crisis is the production of Extended-Spectrum Beta-Lactamases (ESBLs). These enzymes hydrolyze and inactivate most beta-lactam antibiotics, including penicillins, cephalosporins, and monobactams. The sharp rise in third-generation cephalosporin resistance is predominantly caused by different classes of ESBLs like A, C and D.
Five of the seven ESKAPEE pathogens (Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, Enterobacter spp. and E. coli) are Gram-negative bacilli armed with multi-drug resistance (MDR) mechanisms. They are notoriously prominent in complicated urinary tract infections (cUTI), hospital-acquired pneumonia (HAP), ventilator-associated pneumonia (VAP), and complicated intra-abdominal infections.
Because ESBL-producing pathogens often express resistance to other drug classes like fluoroquinolones and aminoglycosides, carbapenems have become the default treatment. However, deploying carbapenems empirically to treat ESBL infections directly drives the emergence of Carbapenem-Resistant Enterobacterales (CRE), a devastating scenario where treatment options are virtually exhausted.
There is a critical need for Carbapenem-sparing options to treat ESBL infections.
The Human and Economic Toll
1.27 M
Deaths directly caused by AMR in 2019, surpassing HIV and Malaria combined.
4.95 M
Projected annual deaths in Asia alone by 2050 if AMR continues unchecked.
$100 to $210 T
The anticipated reduction in global GDP by 2050 due to the economic cost of AMR.
The Scale of the Unmet Clinical Need
The primary clinical battleground for ESBL infections is the urinary tract. Complicated UTIs (cUTIs), which involve structural abnormalities, indwelling catheters, or immunocompromised states, carry a high risk of systemic complications and are the primary target for ESBL-producing pathogens.
~410 Million
Annual UTI cases globally.
~50 Million
Complicated UTI (cUTI) cases requiring aggressive treatment.
~20 Million
ESBL-positive cUTI cases requiring targeted carbapenem-sparing therapy.
THE JOURNEY
A 17-Year Journey from Molecule to Medicine
2006
Enmetazobactam invented by Orchid Pharma.
2010
Patent granted for Enmetazobactam, securing IP protection across 50+ countries.
2006 to 2012
Pre-clinical development for the Cefepime and Enmetazobactam combination.
2013
Licensed the molecule to Allecra Therapeutics for global Phase 2 and 3 development.
2018 to 2020
Completed the ALLIUM Phase 3 trial involving 1,034 patients across 19 countries.
2022
Initiated the AT-202 Pediatric trial in Europe in partnership with ADVANZ Pharma.
2024
Secured quad-regulator approval from USFDA, EMA, UK MHRA, and CDSCO. Launched the Indian brand Orblicef® with Cipla and initiated Phase 4 trials in India for hospital formulary adoption.
2025
Acquired 100% of Allecra Therapeutics. Returned full global ownership of EXBLIFEP®, all regulatory infrastructure, and clinical data to the original inventor.
2030
Anticipated completion of Phase 4 and pediatric trials enabling an expanded global label.
2006
Enmetazobactam Invented
In 2006, a team of chemists and biologists at Orchid Pharma's research laboratories set out to solve a specific and urgent problem of AMR: how to protect beta-lactam antibiotics from ESBL enzymes without losing potency or creating new toxicity.
Their answer was enmetazobactam (formerly known as OCID5090, AAI101), a novel penicillanic acid sulphone beta-lactamase inhibitor (BLI). The critical chemical innovation? Enmetazobactam features an extra methyl group at the triazole ring compared to tazobactam. This structural enhancement allows enmetazobactam to bind tightly to beta-lactamases, preventing the hydrolysis of the antibiotic against Class A, and certain Class D ESBLs, and significantly improving the activity of the associated beta-lactam.
Enmetazobactam, though protects several beta-lactams, Cefepime was chosen to be paired with since it is inherently stable to AmpC class of ESBLs, it is active against Pseudomonas, and also together, they are non-inducers of AmpC.
.webp)
How Does It Work?
Enmetazobactam acts as a shield. It binds to the active site of ESBLs, forming a covalent adduct that neutralizes the enzyme's ability to destroy the antibiotic.
Enzymes active against
Class A and D ESBLs (CTX-M, SHV, TEM, VEB, OXA- type etc).
Enzymes NOT affected
Class B Metallo-beta-lactamases (MBLs).
The targeted spectrum is deliberate, and stewardship driven. Cefepime–enmetazobactam (EXBLIFEP® / ORBLICEF™) is intended as a precision, first-line empiric therapy for suspected ESBL infections, enabling a carbapenem-sparing treatment strategy. By effectively covering ESBL-producing pathogens without unnecessary ultra-broad coverage, it helps preserve carbapenems and other last-line agents for the most resistant infections.
India's First Antibiotic NCE: Enmetazobactam is the first New Chemical Entity (NCE) in the anti-infective space to be invented in India and to receive marketing approval from the USFDA, EMA, MHRA, DCGI, GCC, ANZ, Russia etc. It is a point of immense pride for Indian pharmaceutical science.
2010
The Intellectual Property Fortress
Protecting the invention with IP coverage across 50+ countries.
With the chemical discovery and biological efficacy with safety secured, Orchid Pharma executed a systematic, multi-layered IP strategy designed to protect every commercially relevant dimension of the molecule.
4 Patent Families
Covering Composition of Matter, Method of Use, Polymorph, Process, and Product.
50+ Countries
Providing robust global exclusivity.
77 Jurisdictions
Covered by the Process patent, ensuring the manufacturing route remains protected.
.webp)
This patent protection is reinforced by Orchid's end-to-end control including the supply chain. The complex sterile synthesis required to manufacture these IV antibiotic vials acts as a natural protection, ensuring that only authorized partners can manufacture and supply the product.
2006 to 2012
Early Clinical Development
Why pair enmetazobactam with cefepime? The science behind the combination.
Having invented a potent ESBL inhibitor, the critical question was: which antibiotic should it protect? The answer was cefepime, a fourth-generation cephalosporin.
Reason:
β-lactam antibiotics are frequently compromised by β-lactamase–mediated hydrolysis, particularly from ESBLs (Class A, D) and AmpC β-lactamases (Class C), which inactivate many penicillins and cephalosporins. Cefepime is uniquely advantageous because it is generally stable against hydrolysis by Class C AmpC (both chromosomal and plasmid-mediated) and Class D OXA-type enzymes. Cefepime and Enmetazobactam are zwitter ions and have nearly similar cell penetration, thus facilitating the inhibition+action synergy. Therefore, cefepime already handles major resistance mechanisms on its own, meaning it needs protection against Class A ESBLs.
The Blade (Cefepime)
Exerts bactericidal activity by binding to and inhibiting Penicillin-Binding Proteins (PBPs), inhibiting bacterial cell wall synthesis and leading to cell death.
The Shield (Enmetazobactam)
A potent inhibitor of AMR inducing Extended Spectrum β-lactamases, protecting cefepime from degradation and allowing it to reach its PBP targets fully intact.
Source : Footage from channel SVT; reported by Malin Mendel

2013
Partnering cum Licensing to Allecra Therapeutics
Taking the molecule global through partners.
To conduct the massive, multi-country clinical trials required for approval by the world's most demanding agencies, Orchid Pharma partnered through out-licensing Agreement with Allecra Therapeutics GmbH, a Swiss clinical-stage company.
This strategic partnership deployed Orchid’s molecule into global clinical development under the name EXBLIFEP®, while Orchid retained 18.4% stake, Indian Territory, and IP-linked royalties from global sales
.webp)
2018 to 2020
The ALLIUM Phase 3 Trial
The definitive clinical proof: 1,034 patients, 19 countries, a landmark result.
The ALLIUM trial was a massive, double-blind global study enrolling 1,034 adult patients hospitalized with complicated urinary tract infections (cUTI), including acute pyelonephritis. Patients received either EXBLIFEP® or piperacillin-tazobactam (the current standard of care) via intravenous infusion.
The Results: Statistical Superiority
In the primary efficacy endpoint (clinical cure and microbiological eradication), Cefepime-Enmetazobactam (EXBLIFEP®) demonstrated clear superiority over the standard of care in the mMITT population.
Cefepime-Enmetazobactam (EXBLIFEP®)
79.1%
Piperacillin-Tazobactam
58.9%
Adjusted Difference
+21.2%
The clinical trial, which set out as a Non-Inferiority Trial turned out to be a Superiority Trial based on the above outcome
.webp)
The ESBL-Producing Subgroup:
The superiority was even more pronounced in patients with confirmed ESBL-producing uropathogens, the exact population for which Cefepime-Enmetazobactam (EXBLIFEP®) was built. In this critical subgroup, Cefepime-Enmetazobactam (EXBLIFEP®) achieved a 73.7% success rate compared to just 51.5% for Piperacillin-Tazobactam.
The combination was well tolerated, with a safety profile consistent with cefepime's decades of established clinical use.
2018 to 2020
In-Vitro Surveillance Data
How EXBLIFEP® performs against 9,905 real-world clinical isolates.
Parallel to the Phase 3 trials, extensive in vitro surveillance evaluated the combination against Enterobacterales isolates collected globally.
Against ESBL-positive E. coli, the most prevalent ESBL pathogen globally, the data make the ultimate carbapenem-sparing case:
Cefepime-Enmetazobactam (EXBLIFEP®)
98.1%1 and 98.8%2 Susceptible
Meropenem (Carbapenem)
96.2%1 and 97.6%2 % Susceptible
EXBLIFEP® closes the gap, offering near-perfect efficacy and sparing meropenem for infections that truly require a carbapenem.
.webp)
2022
AT-202 Pediatric Trial Initiated
Extending the science to the most vulnerable patients.
Children are not small adults. To ensure safe and effective dosing from birth through adolescence, Orchid Pharma, in partnership with ADVANZ Pharma, initiated the AT-202 pediatric trial.
This Phase 2, open-label, multi-center study covers 5 age cohorts (from birth to <18 years). While the acquisition led to a temporary halt in 2025, recruitment is planned to resume in 2026 with an expanded site network, pushing toward a highly anticipated label expansion.

2024
Global Regulatory Breakthrough and Clinical Implementation
The year 2024 marked a historic period of regulatory validation for Orchid Pharma. Following the 2023 submission of New Drug Application (NDA) dossiers to four of the world’s most stringent agencies, marketing authorizations were granted with a very short turn-aroundwindow.
This quad-regulator approval confirmed the scientific rigorof Cefepime-Enmetazobactam (EXBLIFEP® globally and ORBLICEF™ in India) for the following:
Approved in
February 2024
Approved in
March 2024
Approved in
April 2024
Approved in
May 2024

In India, the CDSCO fast-tracked this approval by recognizing robust global data and waiving Phase 3 trials. To support wide-scale adoption across Indian hospitals and ensure safety in the Indianpopulation, CDSCO approved Orchid to initiate a Phase 4 Clinical Trial. The clinical scope of the treatment, in addition to cUTI, was further expanded by the EMA based on pharmacokinetic synergy data showing effective concentrations in the lungs, and granted additional approvals for:
Hospital-Acquired Pneumonia (HAP) and Ventilator-Associated Pneumonia (VAP).
Bacteremia associated with cUTI or HAP.
Complicated Urinary Tract Infections with Acute Pyelonephritis
2025
Global Ownership and Clinical Leadership
In a strategically transformative move, Orchid Pharma completed the 100% acquisition of Allecra Therapeutics. This acquisition brought the molecule invented in India back to its original home, granting Orchid full global ownership of:
The complete regulatory infrastructure and commercial rights.
All proprietary clinical data and intellectual property.
Global rights to EXBLIFEP®, returning the invention to its original creator.
.webp)
This leadership was further cemented as the Infectious Diseases Society of America (IDSA) officially recognized the therapy in its 2025 guidelines. The IDSA names Cefepime-Enmetazobactam as a specific empiric and definitive option for cUTI when ESBL-E susceptibility is confirmed. This inclusion solidifies Orchid Pharma’s position at the forefront of the global response to antimicrobial resistance.
2030
The Road Ahead
Pediatric Indication approval, Phase 4 completion, and expanding global access.
The anticipated 2030 completion of the AT-202 pediatric trial and the Indian Phase 4 study marks a critical milestone. A positive pediatric outcome will position EXBLIFEP® as the only approved carbapenem-sparing BLI combination indicated for children with ESBL cUTI from birth.
Where we go from here:
Commercial expansion into key unlicensed markets (US, China, LATAM, GCC, Russia and ANZ).
Additional indication research.
Deepening antimicrobial stewardship partnerships globally.
.webp)
Global Impact
Helping Patients Combat ESBL’s World Over
.webp)
Work on Medicine That Matters
Inventing and developing a new antibiotic is only part of the response to addressing AMR. Ensuring equitable access, stewardship, and sustainability is equally important.
We are actively seeking strategic commercial partners to bring this critical carbapenem-sparing therapy to unmet markets worldwide.
If your organization is aligned with the mission of combating Antimicrobial Resistance through high-value pharmaceutical innovation, we want to partner with you.